TEP 555 Technique
Education event Sponsored by: Medtronic
Conference Name: Advances in Minimally Invasive Hernia Repair
Conducted by: Dr. Vijay Arora,Prof. Brij B Agarwal,Dr. Neeraj Dhamija
Surgeon(s)/Speaker(s): Dr. Manish Gupta
Surgical Procedure: Laparoscopic Hernia-Inguinal Hernias - TEP (totally extraperitoneal)
Location: Sir Gangaram Hospital Delhi
Indexsteps
1. Patient is cathererised : * Patient is cathererised
2. Extraperitoneal approach : * 10mm Infraumbilical transverse incision 1 cm away from midline * Anterior rectus sheath exposed and incised transversely * Stay sutures with 1-0 vicryl on both margins of rectus sheath * Rectus muscle retracted laterally by finger * Space created between muscle and post rectus sheath
3. Ballon dissection of extraperitoneal space : * 2 Finger stalls of No. 8 latex glove fixed over top of suction cannula by thread * Ballon cannula inserted in retroperitoneal space * 100 - 150 ml saline is injected through the cannula to inflate the ballon, kept for 5 minutes * Creates initial space, temporary pressure helps in haemostasis * Blunt tips 10 mm cannula introduced * Insuflation started with a pressure of 12 mm Hg * 10 mm 30 degree telescope passed * 2 other 5 mm working ports placed under vision 2-3 cms above pubic symphysis in midline, midway between 1st and 2nd port
4. Dissection of extra peritoneal space : * Surgeon stands on opposite side of hernia to be separated * Loose areolar tissue plane is dissected in midline with sharp dissectors * 1st landmark in pubic bone as a white glistening structure in midline * Pubic bone dissected free of all connective tissue * Plane is extended for 2-3 cms in retropubic space
5. Lateral dissection : * If hernia is direct type, sac is visualised as a weakness medial to inferior epigastric artery * If hernia is indirect type, vessel is seen before the sac * Sac is reduced by blunt and sharp dissection * Cooper's ligament, iliopubic tract, femoral canal, inferior epigastric artery are visualized * Spermatic cord is inferior and lateral to inferior epigastric vessels * Sac is dissected free (antero lateral to cord) * In indirect type, distal sac is transected * Proximal end ligated using endoloop, distal sac kept open * Vas is seen on medial side and gonadal vessels on lateral side * This is are of triangle of doom (external iliac vessels) * Lateral dissection extended till psoas muscle is seen lying on the floor on which sometimes lateral cut nerve of thigh and genito femoral nerves seen * Anterior superior iliac spine is end point of lateral dissection
6. Introduction of mesh : * Selected polypropelene mesh is rolled like a cigar and inserted through the 10 mm port * Mesh is spread covering direct, indirect, femoral obturater hernia sites * Mesh is spread adequately covering from midline medially, laterally upto psoas muscle * Under vision 5 mm ports are removed and peritoneal space deflated taking care that mesh does not fold * 10 mm port is removed * All ports are closed
7. Bilateral hernias : * In case of bilateral hernias, similar procedure as given above should be done on both sides through the same ports
port positions
1. Port positions-TEP : * 10mm infraumbilical transverse incision 1 cm away from midline
* 10 mm 30 degree telescope used
* 2 other 5 mm working ports placed under vision 2-3 cms above pubic symphysis in midline, midway between 1st and 2nd port.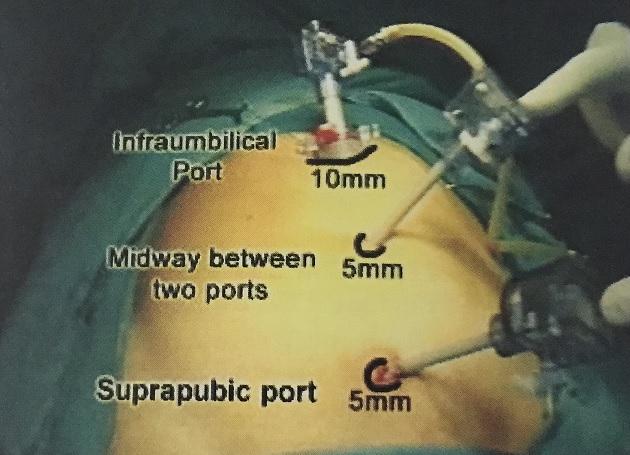
precautionary_measures
1. Complete reduction of the sac should be avoided : In case of complete hernia, complete reduction of the sac should be avoided as it can cause postoperative pain
2. Dissection : No dissection should be done in the triangle of doom as it contains the external iliac vessels
pre_post_measures
1. Preoperative investigations : CBC:new:X-Ray Chest:new:ECG:new:Coagulation profile:new:Pulmonary function test
2. Preoperative measures : Fasting for 8 hours
3. Postoperative measures : NBM for 6 hours:new: Ambulate after that:new: Two dose of Antibiotics:new: Analgesics as required:new:
4. Warning signs in the postoperative period : Careful closure of the fascia at the umbilical trocar site:new: Infiltration of all trocar sites with local anesthetic:new: Closure of wounds and application of dressing:new: Pressure dressing is given on the Inguinal area to reduce Seroma.:new:
Surgical Instruments
1. Absorba Tack Fixation Device
2. Symbotex composite mesh
3. Dextile Anatomical Mesh
4. Parietex 3D Mesh
5. 10mm Trocar
6. Vessel Sealer
7. Polypropelene Mesh
8. Suture
9. Retractors